



Description
Course type: Online; Self-Paced
Specialty: Specialty: Cardiology
Language: English, Portuguese
Resources: Debriefing Videos
Level: Intermediate / Advanced
Target: General Practitioner and Hospital Care Physicians
Modules: 10
Durations: 2 months
Time Effort: Up to 110 minutes per module
Certificate: Yes
Course Description
Heart failure is a clinical syndrome caused by structural and/or functional cardiac abnormality, leading to reduced cardiac output and/or elevated intracardiac pressures at rest or during stress.
CHeFS – Comprehensive Heart Failure Simulations course allows, through simulation with virtual patients, to establish the best therapeutic approach according to the best available evidence.
This course is based on evidence-based practice recommendations, focused on the diagnosis and treatment of HF, including explanatory videos enhancing learning.
Course Overview
- 10 Modules
• 10 virtual patient cases of an intermediate level of complexity - Average Time to practice (per module):
• Clinical Scenario: 20 minutes per attempt (3 attempts: 60 minutes)
• Final attempt (if applicable): 20 minutes
• Multiple Choice Question: 5 minutes
• Feedback Area: 10 minutes
• Learning Objectives and Scientific References: 10 minutes
• Debriefing Video: 10 minutes - Online, Self-paced
• You have up to 2 months to complete the 10 modules at your own pace. The course can be accessed through Body Interact at any time. - Certificate of Completion
• After completing the course, you will receive a Certificate of Completion that can be added to your CV or Resume.
Learning Objectives
• Diagnose and risk-stratify acute chronic heart failure
• Distinguish between heart failure with preserved and reduced ejection fraction
• Optimize medical treatment for all heart failure patients
Clinical Competencies
Safety
• Collect patients’ clinical information
• Establish drug dosing for common medications
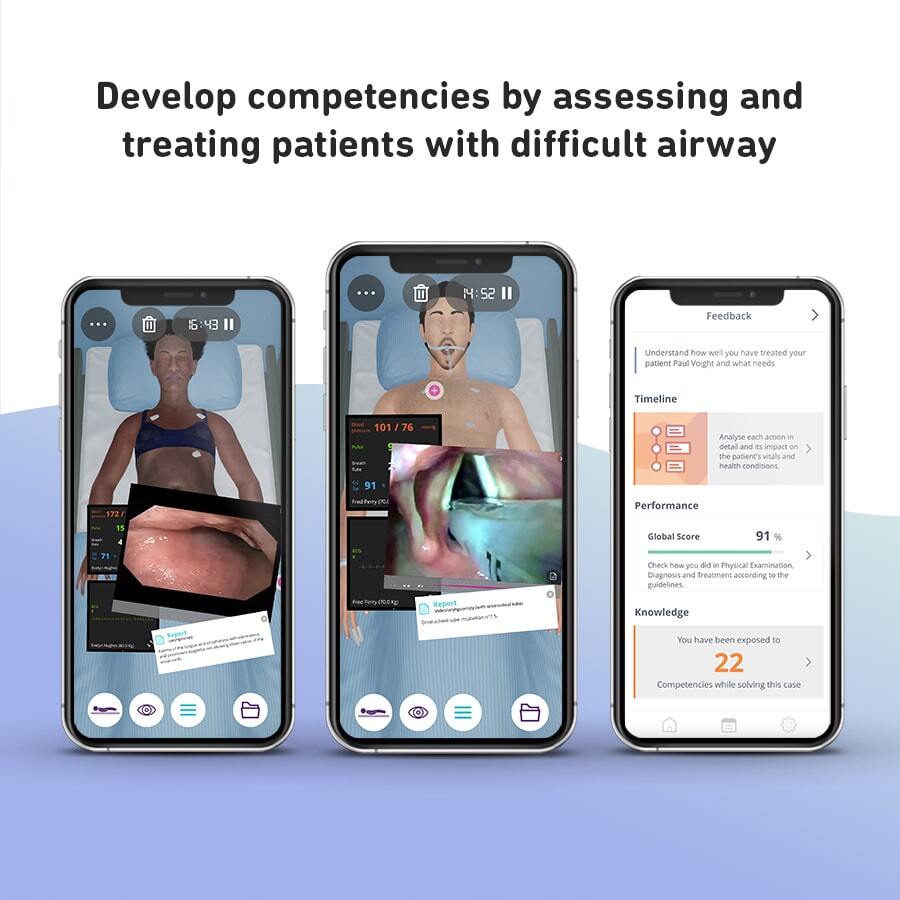
Airway and Breathing
• Basic airway management
• Lung examination (percuss, fremitus, auscultation and qualities of air sound, lobar locations)
Circulation
• Assess and interpret blood pressure (various sites and body positions)
• Assess and interpret pulse (rate, rhythm and volume)
• Detect heart murmurs
Disability
• Blood sugar measurement and interpretation
• Mental status examination
Exposure
• Abdominal plain x-ray interpretation
• Arterial blood gas interpretation
• Assess and interpret temperature
• Assess height and weight
• Cardiac enzyme interpretation
• Cath lab techniques interpretation
• Catheter management
• Central venous catheter placement
• Chest x-ray interpretation
• Cornea and anterior chamber assessment
• Cranial nerves assessment
• Disc (color, edges, size and shape) examination
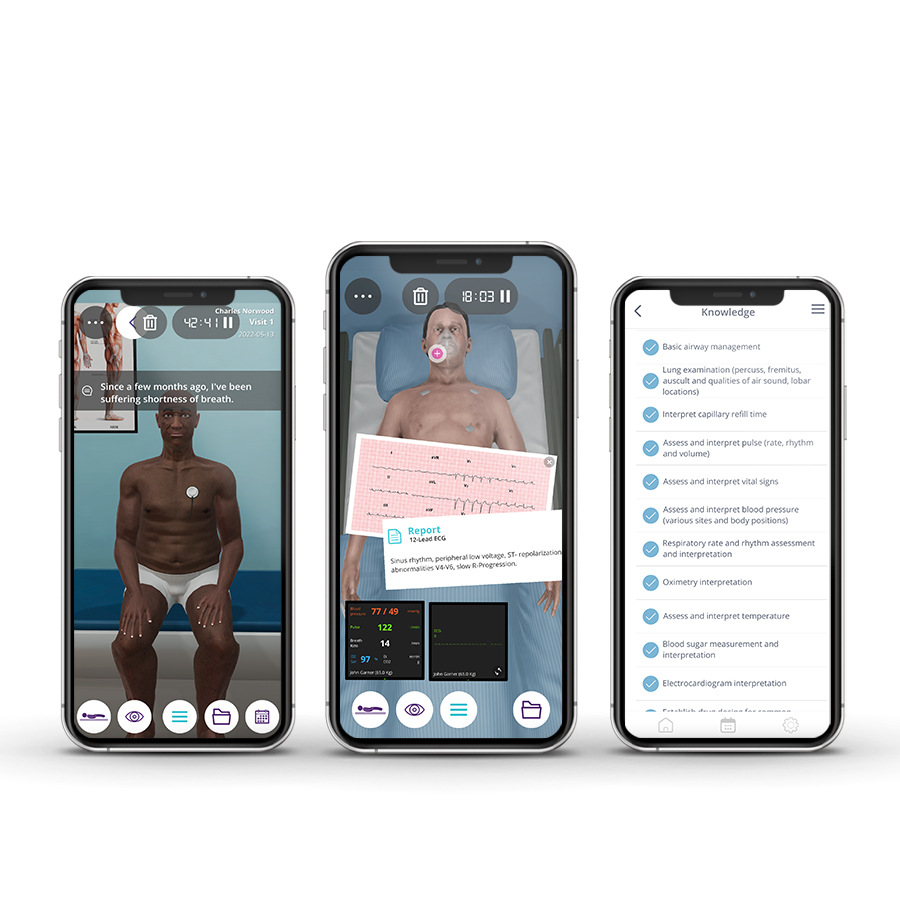
• Electrocardiogram interpretation
• Fluid/Electrolyte test interpretation
• Gait and station assessment
• Hand and foot examination
• Hematocrit interpretation
• Lens (clarity, artificial iol) examination
• Motor function (voluntary movements, reflex withdraw, spontaneous, involuntary movements, tone)
• Nutrition management
• Lipid test interpretation
• Liver function test interpretation
Module 1 – The new age of chronic heart failure
Context: Modern heart failure management often requires upgrading medical therapy in patients that still have symptoms. The new guidelines help us improve the clinical condition and prognosis of those patients.
Virtual Scenario: Mr. Liu has recently retired from his job. He has been losing his energy with small efforts at home, going up and down the stairs. He also has a medical history of alcoholism and smoking.
Module 2 – Is three too much or not enough?
Context: Modern heart failure management often requires upgrading medical therapy in patients that still have symptoms. The new guidelines help us improve the clinical condition and prognosis of those patients, even if they are on triple therapy.
Virtual Scenario: Ms. Wilkins hasn’t been feeling well lately. Daily tasks seem to leave her without any energy, even before completing them. A family member recommended she see a doctor, which is why she is here at the clinic.
Module 3 – Fantastic four
Context: Modern heart failure management often requires upgrading medical therapy in patients that still have symptoms. The new guidelines help us improve the clinical condition and prognosis of those patients, even if they are on suboptimal medical therapy.
Virtual Scenario: Mr. Reed really enjoys socializing with his friends. He has dinner with his friends every week, but at his last dinner, his colleagues noticed that he felt very tired and with shortness of breath when he made small efforts. They talked to him and he made a routine appointment.
Module 4 – Is normal really normal?
Context: Is shortness of breath always a heart condition? This case allows us to assess differential diagnosis and identify cardiac patients in need for optimizing optimal therapy
Virtual Scenario: Mr. Norwood has recently been feeling unwell. He often gasps for air when going for a walk. Concerns for his health started to settle in, and he decided to seek medical care.
Module 5 – A blank page, a falling heart
Context: When we have a patient with a recent diagnosis of heart failure, which should be our priorities? Which exams should be ordered? Which drugs should be started?
Virtual Scenario: Mr. Wongwirot has not been very much concerned with his health. Instead, his social and economic situation preoccupied him during the past decades. Consequently, this man has struggled to provide for his family for most of his life. However, it took its toll on his health.
Module 6 – Beyond water
Context: Diuretics make the patient feel better, with less dyspnea and fatigue. Does this mean that diuretics are all it takes to improve patient prognosis?
Virtual Scenario: Mr. Churo has been feeling poorly for most of the last year. However, he firmly believes in being autonomous and independent. Consequently, he has stubbornly refused his family’s pleas to see a doctor. That is, until now.
Module 7 – 20 minutes to the end
Context: Severe dyspnea, no pulse, no urinary output. Is this the end? Or can we rapidly do something about it?
Virtual Scenario: Mr. Garner initially collapsed on the street and was resuscitated. He was presented with coronary artery disease (acute occlusion of the prox. LAD and RCX) with severely depressed ejection fraction, EF=30% by echocardiography. The patient presented with severe and persistent cardiogenic shock.
Module 8 – How to deal with a little drama?
Context: In heart failure, a few days can make all the difference. Swollen legs, shortness of breath, another visit to the ER. Can we change the patient’s outlook?
Virtual Scenario: Mr. Perry reports he has been getting more short of breath from walking across the room and has to sleep in a recliner. He has gained considerable weight over the past 3 weeks. He noticed a little chest pressure yesterday, which has resolved. He continues to be substantially short of breath.
Module 9 – Is sugar the answer?
Context: Diabetes and heart failure often go hand to hand. However, if a heart failure patient is not diabetic can we still benefit from sugar-lowering drugs?
Virtual Scenario: Mr. Pollard came to the emergency room with complaints of easy fatigue and dyspnea on moderate effort with two weeks of evolution that worsened today.
Module 10 – Getting into reason
Context: For heart failure patients everything can be a game-changer. Can a cardiac arrhythmia spell the end for this lady?
Virtual Scenario: Ms. Harris came to the emergency room with complaints of easy fatigue and dyspnea on moderate effort with four weeks of evolution that worsened today.
Authors and Speakers
With a multidisciplinary group of international clinical reviewers, Body Interact ensures a high standard of accuracy, diversity, and impact of its course.
Pedro Monteiro
MD, PhD
Faculty of Medicine, University of Coimbra, Portugal
Cardiology Consultant – Coimbra University Hospital
Scientific References
- McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: Developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) With the special contribution of the Heart Failure Association (HFA) of the ESC. European Heart Journal. 2021;42(36):3599-3726.
- Yancy Clyde W., Jessup Mariell, Bozkurt Biykem, et al. 2017 ACC/AHA/HFSA Focused Update of the 2013 ACCF/AHA Guideline for the Management of Heart Failure. Journal of the American College of Cardiology. 2017;70(6):776-803.
- Gaddam KK, Ventura HO, Lavie CJ. Metabolic syndrome and heart failure–the risk, paradox, and treatment. Current Hypertension Reports. 2011;13(2):142-148.
- Heidenreich PA, Bozkurt B, Aguilar D, et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145(18).
- Valerino-Perea S, Lara-Castor L, Armstrong MEG, Papadaki A. Definition of the Traditional Mexican Diet and Its Role in Health: A Systematic Review. Nutrients. 2019;11(11):2803.
Body Interact – This course is based on the most recent guidelines, using advanced medical simulation technology with virtual patients.
Recommendations
Explore more related courses by Body Interact
-

 Medical
Medical -
 Medical
Medical -
 Medical
Medical -
 Medical
Medical -
 Medical
Medical -
 Medical
Medical